

Naltrexone: A Potential Emerging Therapy for Pornography Addiction
Porn addiction is a rapidly growing concern, with the increased access and seemingly unlimited digital reach of online content contributing to this trend. Despite being a controversial subject, pornography addiction has been identified as a behavioral addiction, with individuals struggling to control their pornographic use. Porn addiction can have considerable negative consequences on relationships, mental health, and overall well-being. Recent research (referenced below) suggests that Naltrexone, a medication commonly used to treat alcohol and opioid addiction, may be an effective treatment for porn addiction when coupled with individual and group therapy - additional research is needed. This post will examine the advantages and disadvantages of using Naltrexone as a potential treatment for pornographic addiction, as well as its potential efficacy in assisting individuals in overcoming this addiction.
Online pornography and cybersex addiction is a growing problem in the digital age, and it can have severe effects on individuals and their relationships. In this post, I will discuss the case study of an individual who sought assistance for porn addiction, and other online compulsive sexual behavior, and outline their experience with the medication Naltrexone.
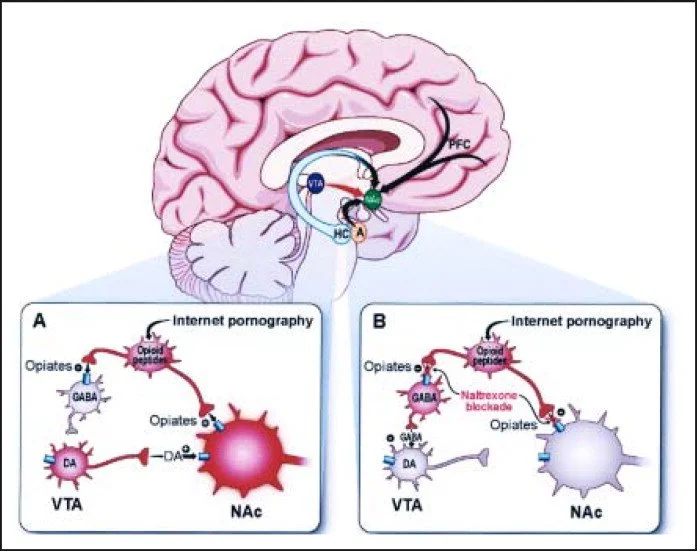
First, it is essential to comprehend how addiction functions in the brain. Addiction is not simply a matter of lack of willpower or moral deficiency; it is the result of a complex interaction between brain chemistry and behavior. In online pornography and cybersex addiction, the brain's reward system, specifically the nucleus accumbens (NAc) and ventral tegmental area (VTA), becomes dysregulated. The release of the neurotransmitter dopamine, which is associated with pleasure and reward, is controlled by these regions of the brain. The NAc participates in the processing of reward, motivation, and pleasure, whereas the VTA is a key component of the brain's reward system, playing a central role in the experience of pleasure and the reinforcement of behavior. It is essential to note, however, that the brain's reward system is complex, involving multiple regions and neurotransmitters, and that the concept of a single "pleasure center" oversimplifies this complexity.
Normally, motivationally relevant events (MREs) such as hunger or sexual arousal trigger the brain's reward system. These occurrences cause the release of endogenous opiates (endorphins), which in turn causes an increase in dopamine levels. The reward system of the brain responds to an event with a motivated action behavior (MAB) and cellular changes that encode long-term learned associations with the event. These neuroplastic changes result in a more rapid behavioral response when the event recurs, and repeated MRE exposure typically attenuates and eventually eliminates dopamine release in the VTA.
However, addictive substances and behaviors affect the reward system of the brain differently than MREs. Repeated exposures to addictive substances or behaviors do not extinguish dopamine release; in fact, drugs can outcompete natural stimuli by eliciting significantly more dopamine release for longer durations. This results in a vicious cycle of addiction in which the continued release of dopamine assigns increasing importance to drug-seeking and diminishing importance to behaviors fundamental to normal function and survival.
In the case of the case study being discussed here, the individual had developed an addiction to cybersex and online pornography, which caused him to spend hours per day engaging in these activities. His inability to control his behavior was beginning to affect his personal and professional life. He worked with a prescribing physician who decided to add naltrexone to his regimen of medications, which already included an SSRI.
Naltrexone is a medication that blocks morphine receptors, resulting in a direct and indirect increase in GABA tone and a decrease in NAc dopamine levels. This interrupts the unrestrained dopamine crescendo that leads to an imbalance in the salience attribution and response inhibition functions. Eventually, through gradual desensitization, the salience of the addictive behavior should diminish.
In the case of this case study, the individual saw the addition of naltrexone to his medication regimen as being contemporaneous with a precipitous decrease in his addictive symptoms. He no longer found his online sexual activities irresistibly rewarding, and the salience of the cues prompting these activities decreased to the point of the behavior's abatement. He discovered, coincidentally but not unexpectedly, that he no longer enjoyed binge drinking.
Additional studies are cited below, as well as reference material, however, this case study illustrates the potential efficacy of naltrexone in treating addiction to cybersex and online pornography. To confirm that these observations can be generalized to other individuals and to clarify the mechanism by which naltrexone eradicates addictive behavior, additional research is required. Several published case reports (below), however, have demonstrated its potential for treating other addictive behaviors, including pathologic gambling, self-injury, kleptomania, and compulsive sexual behavior. Repeatedly engaging in a behavior or activity can lead to changes in the reward system of the brain, known as the incentive salience circuit (ISC). Typically, the ISC responds to motivationally relevant events (MREs) such as hunger or sexual arousal by releasing endogenous opiates (endorphins) that cause an increase in dopamine levels. The ISC responds by encoding long-term learned associations with the MRE, resulting in a quicker behavioral response when the event recurs. Repeated exposure to MREs attenuates and eventually eliminates VTA dopamine release, indicating that dopamine release is no longer required for survival-related behaviors.
However, addictive substances and behaviors have distinct effects on the ISC. Dopamine release is not extinguished by repeated exposure, and these substances can outcompete natural stimuli by inducing significantly more dopamine release for longer durations. This vicious cycle results in a continuous release of dopamine, which assigns increasing importance to drug-seeking and diminishing importance to behaviors vital to normal function and survival. In drug addiction, the ability to assign an appropriate value to the drug and the ability to resist its siren call, both frontal lobe functions, become aberrant. As a result, addicts may neglect their children, commit crimes, or continue their compulsive behavior despite suffering from painful illnesses.
Pharmacotherapies such as Naltrexone can help interrupt the unrestrained dopamine crescendo that leads to an imbalance in the functions of salience attribution and response inhibition. Naltrexone is a morphine-receptor antagonist that blocks morphine receptors, thereby increasing GABA tone and decreasing NAc dopamine levels via direct and indirect mechanisms. Eventually, through gradual desensitization, the salience of the addictive behavior should potentially diminish. In addition to the Food and Drug Administration's approval of Naltrexone for the treatment of alcoholism, several published case reports demonstrate its potential for treating pathologic gambling, self-injury, kleptomania, and compulsive sexual behavior.
Two recent research studies:
In 2003, the Journal of Clinical Psychopharmacology published the initial study. A randomized, double-blind, placebo-controlled study examined the efficacy of naltrexone in the treatment of hypersexual disorder (sex addiction). Participants in the study were required to meet the criteria for hypersexual disorder, which included experiencing distress due to their sexual behavior and engaging in prolonged sexual activities. The study found that naltrexone was effective at alleviating hypersexual disorder symptoms. Those who received naltrexone reported significantly fewer sexual thoughts, fantasies, and behaviors than those who received a placebo.
In 2017, the Journal of Addiction Medicine published the results of the second study. It was a case series that examined the use of naltrexone to treat sexual addiction. Participants in this study all reported compulsive porn use symptoms, including using porn more frequently than intended, spending excessive amounts of time watching porn, and experiencing negative consequences in their personal and professional lives as a result of their porn use. The study found that naltrexone effectively reduced the participants' pornographic cravings and the amount of time they spent watching pornographic content. Participants also reported a reduction in anxiety and depression symptoms.
Overall, these studies indicate that naltrexone may be an effective treatment option for those with hypersexual disorder or pornographic addiction. To fully understand the potential benefits and drawbacks of naltrexone for these conditions, however, additional research is required.
Additional research is required to confirm that the above-referenced findings can be generalized to others and to elucidate the mechanism by which naltrexone eradicates addictive behavior. Nonetheless, the potential benefits of using Naltrexone to treat addictive behaviors are encouraging and can offer hope to those who are battling porn addiction, sex addiction, or compulsive sexual behavior disorder.
Naltrexone is only intended for short-term use. In addiction treatment, Naltrexone is typically prescribed for short-term use of less than three months. Long-term use of the medication can result in liver damage. In addition, long-term use can reduce the body's natural endorphin production, resulting in withdrawal symptoms when the medication is discontinued. Naltrexone should only be used under the supervision of a prescribing physician, as it can interact with other drugs and cause side effects. Patients should be closely monitored for potential adverse effects and should not abruptly stop taking the medication without consulting a physician.
In conclusion, although Naltrexone has demonstrated promising results in the treatment of addiction, however, if prescribed it should only be used for a brief duration under the supervision of a healthcare professional in order to minimize the risk of adverse side effects. Common naltrexone side effects include nausea, headache, vertigo, fatigue, and insomnia. Some individuals may also experience more severe side effects, such as liver damage, allergic reactions, or psychiatric symptoms such as depression or suicidal ideation. Before beginning any medication, including naltrexone, it is essential to consult a healthcare professional to discuss the potential risks and benefits and to determine if it is the best option for you. In addition, it is essential to adhere to the prescribed dosage and to inform your healthcare provider of any adverse effects.

References:
Koob, G. F. (1992). Anatomy, pharmacology, and function of reward pathways in relation to drugs of abuse. 13(5):177-184. Trends in Pharmacological Sciences.
Pettit, H. O., Ettenberg, A., Bloom, F. E., & Koob, G. F. (1984). The destruction of dopamine in the nucleus accumbens inhibits rats' self-administration of cocaine but not heroin. Psychopharmacology, 84(2), pp. 167-173, 1999.
Volkow, N. D., Fowler, J. S., Wang, G. J., & Swanson, J. M. (2004). Dopamine in substance abuse and addiction: imaging results and treatment implications. 9(6) Molecular Psychiatry, 557-569.
Hyman, S. E., & Malenka, R. C. (2001). The neurobiology of compulsion and its persistence in relation to addiction and the brain. Nature Reviews Neuroscience, 2(10), p. 695 - 703.
Hyman, S. E. (2005). The disease of learning and memory is addiction. 1414-1422 in American Journal of Psychiatry, 162(8).
Everitt, B. J., & Robbins, T. W. (2005). From actions to habits to compulsion: the neural systems of reinforcement in drug dependency. Nature Neuroscience, 8(11), 1481-1489.
Kalivas, P. W., & Volkow, N. D. (2005). Pathology of motivation and choice as the neural basis of addiction. 1403-1413 in American Journal of Psychiatry, 162(8).
Grant, J. E., Kim, S. W., & Potenza, M. N. (2003). Pharmaceutical advances in the treatment of pathological gambling. 19(1) Journal of Gambling Studies: 85-109.
Koob, G. F., & Le Moal, M. (2005). The relationship between the plasticity of reward neurocircuitry and the "dark side" of drug addiction. Nature Neuroscience, 8(11), 1442-1444.
Childress, A. R., A. V. Hole, R. N. Ehrman, S. J. Robbins, A. T. McLellan, and C. P. O'Brien. Cue reactivity and interventions for cue reactivity in drug dependence. 137 NIDA Research Monograph: 73-95.
Breiter, H. C., Gollub, R. L., Weisskoff, R. M., Kennedy, D. N., Makris, N., Berke, J. D., ... & Hyman, S. E. (1997). Neuron, 19(3), pp. 591-610: Acute effects of cocaine on human brain activity and emotion.
Bolla, K. I., D. A. Eldreth, E. D. London, K. A. Kiehl, M. Mouratidis, C. Contoreggi,... & M. Ernst (2003). A dysfunction of the orbitofrontal cortex in abstinent cocaine abusers performing a decision-making task. Neuroimage, 19(3), 1085-1094.
Christie, M. J., & Osborne, P. B. (1994). Opioid receptors in the brain of mammals. Molecular Neurobiology, 9(1-3), 1-11.